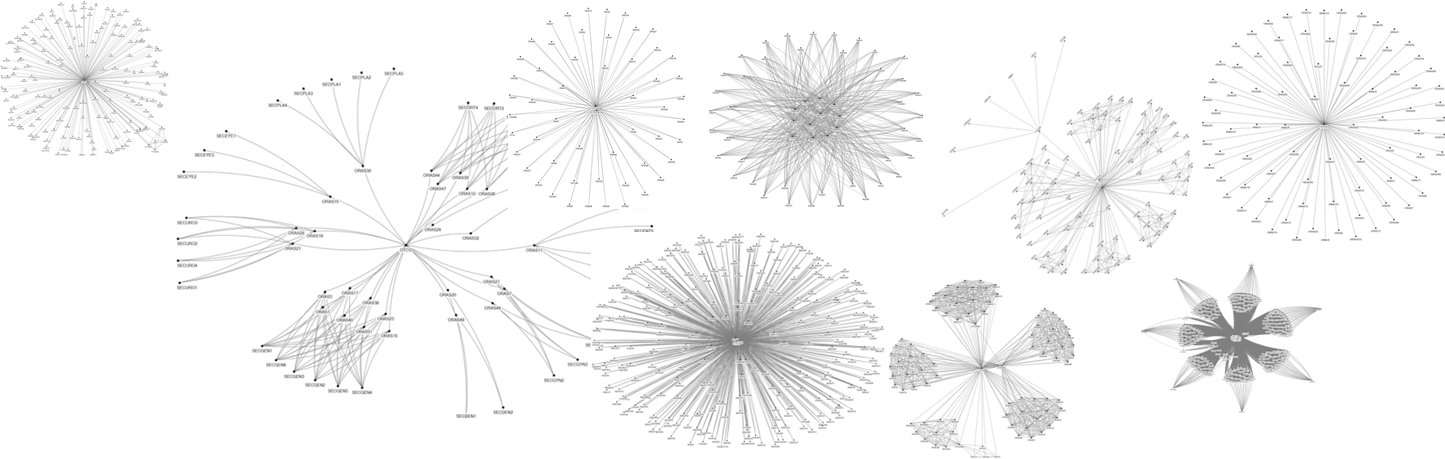
Happy new year! These fireworks are in fact nine social networks for nine tasks that are performed in order to do surgeries for patients. The entire network in my previous blog is built up from 23 social networks, one for each task. Tasks are for example: making the master schedule for the operating theatre (OT), admitting the patient to the ward or performing the surgery. The networks shown here all show centralization. Centralization is the extent to which a set of people are organized around a central person. This is seen in the networks here as one or a few persons in the middle, surrounded by people who interact with the central person(s).
You might expect that these central persons have a hierarchical position towards the others; that they are the boss who ask or instruct people to do things. This is not the case. In most cases in these networks the persons in the middle have no hierarchical position towards others whatsoever. The central people in the networks shown here are the OT day coordinator and the OT capacity planner, logistical staff, secretaries and nurses. In fact the people who do have formal power, in the organizational structure of the hospital, do not have central positions in the operational system of the hospital I studied.
So, not only is the hospital run by people in the operational system itself – mainly by nurses -, it appears that the operational system functions largely on its own, independent or loosely connected to management. This reminds me of one of my first blogs in which I was amazed at the unexpected and undesirable outcomes of strategic transformations of hospitals. I am wondering if it is true that management knows so little about how the operational system works that strategic decisions can lead to unpredictable outcomes. They are not able to observe the operational system and data on the operational system do not always seem to represent reality (see previous blog). This has little to do with competence, but rather with the impossibility to oversee the operational system. And perhaps this applies to all of us, people not working in this operational system. And does it also work the other way around? Do people working in the operational system know what other interests (financial, legal, ethical, technological etc etc.) are at stake besides treating the patient? I think connecting the strategic and operational reality is one of the most important challenges of our time. In 2019 I will make a further attempt to make some kind of contribution to that.